What is percutaneous nephrostomy?
Kidneys are organs in the abdomen which filter the blood and discard the unwanted salts and other products, which are excreted in the form of urine. The kidneys are connected to the urinary bladder (an elastic bag) in the pelvis via tubes called the ureters. Sometimes these tubes get blocked. Due to this blockage, the urine cannot go into the bladder. This creates three problems; one is pain and discomfort which can be felt in the back at the lower end of the ribs transferring all the way in the front near the groin. The second problem is stress on the kidney which causes acute or chronic kidney failure. The third problem is a urinary infection, which can present as fever and chills, or loss of blood pressure if severe.
Obstruction can be caused primarily by three causes. First, a stone in the ureter which causes a block. Second, a tumour (cancer) within the urinary system, either in the ureter, bladder or prostate. Third, a cancer outside the urinary system compressing the ureter.
Solution that can be offered
A double J stent placed by your urologist. Here, the urologist passes a camera into the bladder, visualizes the entry of the ureter into the bladder, and passes a plastic tube that is curved like a J at both ends (hence double J) in under X-ray guidance. One end remains in the kidney, and the other in the bladder, which helps the urine descend into the bladder around the obstruction.
The second option: Percutaneous nephrostomy
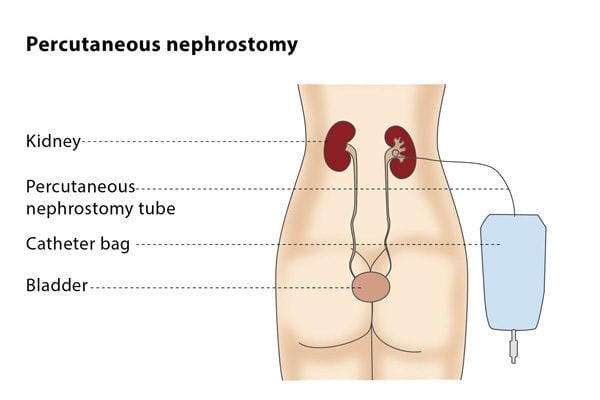
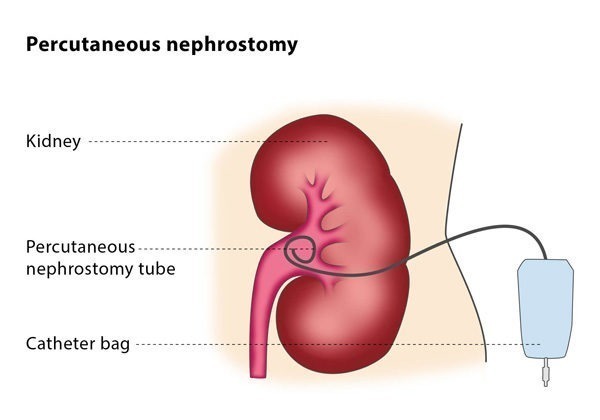
Sometimes, if urologists are not able to pass the tube via the bladder or think it is not a good idea, they recommend a percutaneous nephrostomy. A nephrostomy tube is a thin, flexible tube with resembles a pig’s tail on the inside. The outside looks like a straight plastic tube coming out of the skin in the region of your flank. This tube will be connected to a plastic bag (urine bag). The tube is fixed to the skin with a skin suture. You may also find a butterfly-like dressing holding it in place. You will have a skin dressing over it. Urine leaving the kidney is collected in a plastic bag attached to the tube outside your body. The bag can be strapped to your waist or leg so you can move freely. Once the catheter is in place, you will get pain relief, and if your kidney function is altered, you will notice improvement of the kidney function to how it was before the obstruction happened.