Why perform it?
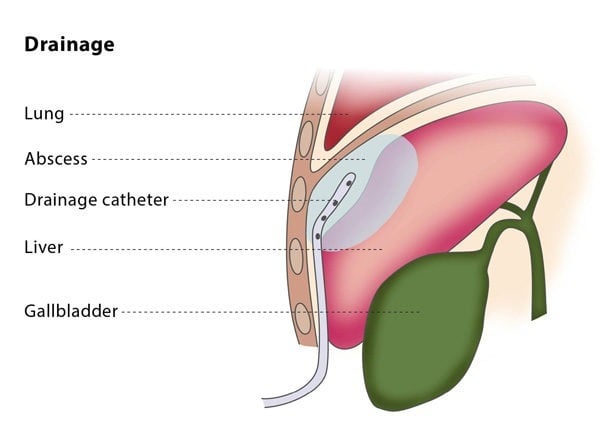
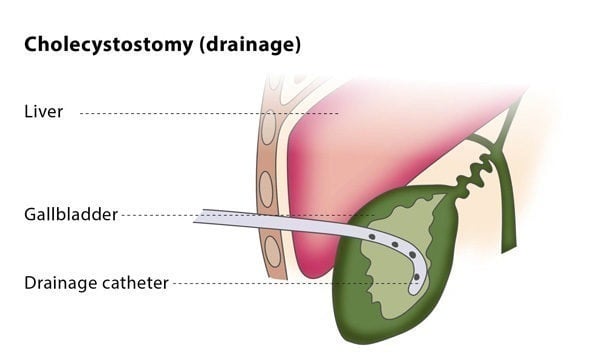
Percutaneous drainage is recommended to treat fluid or air collections which produce symptoms (such as pneumothorax, which is the collection of air or gas in the gap between the chest wall and the lungs). It can also treat recurrent fluid collections by using medication and is a minimally invasive method of draining abscesses.
This procedure may not be suitable for you if you suffer from a blood clotting disorder or if the interventional radiologist cannot find a safe access route for the catheter.
The percutaneous drainage procedure cures infected fluid/air collections in over 80% of patients, though failure occurs in 5-10% of patients.
Because of the wide range of types of uninfected collections, the success rate of drainage for uninfected collections is highly variable.
What are the risks?
There are some risks associated with the procedure. Major complications include bacteraemia (the presence of bacteria in the blood, which occurs in 2-5% of cases) and septic shock (caused by severe infection and sepsis, which occurs in 1-2% of cases). Other complications include the risk of haemorrhage and superinfection (infection of a sterile collection of fluid, following a previous infection).
Bibliography
1. Bakal CW, Sacks D, Burke DR, Cardella JF, Chopra PS, Dawson SL, Drooz AT, Freeman N, Meranze SG, Van Moore A Jr, Palestrant AM, Roberts AC, Spies JB, Stein EJ, Towbin R; Society of Cardiovascular and Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for adult percutaneous abscess and fluid drainage. J Vasc Intervent Radiol 1995; 6:68-90.
2. Silverman SG, Mueller PR, Saini S, et al. Thoracic empyema: management with image-guided catheter drainage. Radiology 1988; 169:5-9.
3. Van Sonnenberg E, D’Agostino HB, Casola G, et al. Lung abscess: CT-guided drainage. Radiology 1991; 178:347-351.