What is stenting?
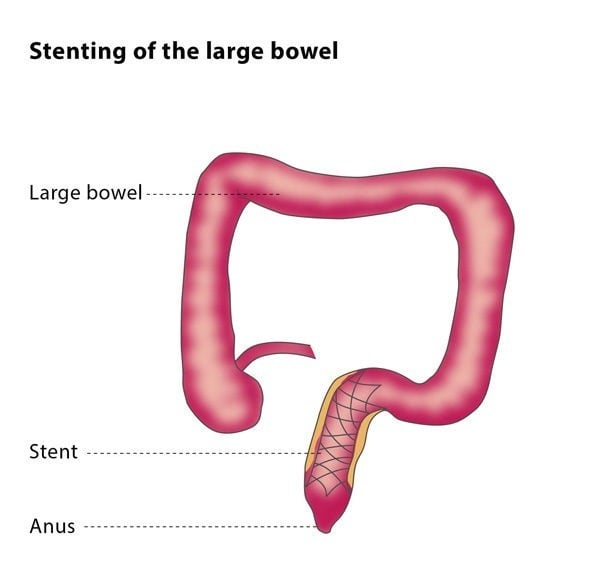
Stenting is the placement of a stent inside your body. A stent is a mesh tube made out of metal, or sometimes out of plastic or silicone, which can be inserted into a hollow tube-like organ in the body (in this case, the food tract) to act as a support scaffold and keep it open. You may be advised to have a stent placed if you have a blockage in your gullet or bowel which is caused by a tumour or by a stricture. A stricture is a narrowing caused after an operation or radiotherapy, or sometimes after the ingestion of some chemicals.
Symptoms of a blockage in the gullet, stomach or small intestine include being unable to consume an adequate amount of food, nausea and vomiting. If you have a blockage in your large intestine, you may find it difficult to go to the toilet. Other symptoms include bloating or severe weight loss, if you are unable to eat.
A stent may also be used to close a fistula. A fistula is a hole between different compartments of the body which should not exist. A fistula may be due to cancer or may happen after surgery, endoscopy, or trauma.
How does the procedure work?
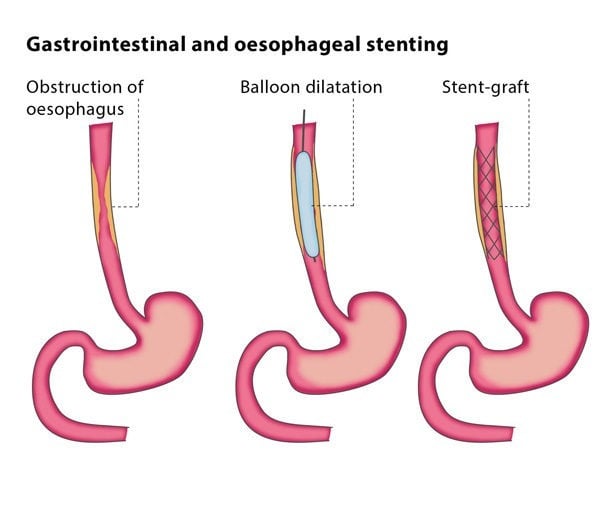
Before the procedure, the interventional radiologist will outline the obstruction with contrast material under X-ray. You will have a local anaesthetic in your throat and be under mild sedation or general anaesthesia for the procedure. The interventional radiologist will introduce a device containing a wire and a catheter (a thin plastic tube) through your mouth and to the blockage in your gullet or small intestine. The catheter and wire will be used to go past the narrowing or region of the fistula. Once the wire is past the region of interest, the catheter will be removed, and a balloon will be inserted over the wire up to the region of interest. The balloon is then expanded to open the passage prior to stent placement. If under conscious sedation, this is the point where you might feel some discomfort or pain. The anaesthetist on site can give you more medications if need be.